
A study recently published in Research Connections drew attention for finding very high rates (relatively speaking) of puberty-blocker and cross-sex hormone uptake among adolescents in Oregon. A separate insurance database analysis by the Manhattan Institute, published here for the first time, adds further detail, suggesting that Oregon has become a national leader in transgender diagnoses and medical intervention. Not coincidentally, Oregon is the only state in the country to have formally adopted the World Professional Association for Transgender Health’s recommendations as the basis for its Medicaid benefits. And it did so despite its own health regulatory body acknowledging the absence of supportive evidence.
Using insurance data for minors ages 8 to 17 between 2016 and 2023, the authors of the recent Research Connections study found that about one in 240 girls and one in 630 boys in Oregon were on hormones by age 17. In addition, 0.98 percent of minors—1.51 percent of girls and 0.46 percent of boys—received a “transgender-related diagnosis” (typically “gender dysphoria”) during these years. In other words, about one in every 65 adolescent girls in Oregon is a potential candidate for medical “sex reassignment.” Also of note, the median age of diagnosis in the study was 14 for both boys and girls, and the median time from diagnosis to medical intervention was just under ten months—findings consistent with the rapid-onset gender dysphoria (ROGD) presentation,
Finally, a reason to check your email.
Sign up for our free newsletter today.
To put these figures into context, when the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) was published in 2013, it reported a diagnostic prevalence of gender dysphoria among adults as 0.002 percent to 0.003 percent for females and 0.005 percent to 0.014 percent for males. Even if we assume (incorrectly) that gender dysphoria is a single clinical entity, this means that diagnosed teen girls and boys in contemporary Oregon thus represent a rise of, respectively, more than 500 and 30 times the prevalence of pre-2013 figures.
Hormonal prescriptions in Oregon have also outpaced the already-rising national average. Last year, a study published in JAMA Pediatrics reported that approximately one in 1,000 American teens was prescribed cross-sex hormones by age 17. The Oregon rate was two to three times higher than that. Indeed, a closer look at the data revealed that hormone prescriptions in Oregon were four to five times the national rate among 14- and 15-year-olds, while puberty-blocker uptake was up to six times the national rate at age 14. Thus, teens in Oregon are not only being medicalized more, but also at earlier ages.
Crucially, the Research Connections authors also note that the percentage of teens in Oregon receiving a clinical diagnosis was only “slightly lower” than the percentage of teens who socially identify as transgender—a very significant finding whose importance the authors, likely because of their positive view of the “gender-affirming” approach, fail to grasp. I elaborate on this below, but for now, it suggests that a social identity is a short step from a diagnosis, which opens the door to a variety of insurance-covered medical interventions including surgeries.
As significant as the Research Connections findings are, they do not tell the whole empirical story. A few years ago, the Manhattan Institute obtained a national all-payers, all-claims insurance database covering the years 2017 to 2023—almost exactly the time frame of the Research Connections study. Our database has enabled us to estimate the incidence of gender-transition double mastectomy (“top surgery”) among teen girls (a bare minimum of 5,200 procedures during those years) and the persistence of transgender-related diagnoses (most adolescents lost the diagnosis within seven years).
The publication of the new Oregon study has given us reason to go back to our database to see how the findings in the Research Connections compare to our data for Oregon and other states when it comes to trends in diagnoses.
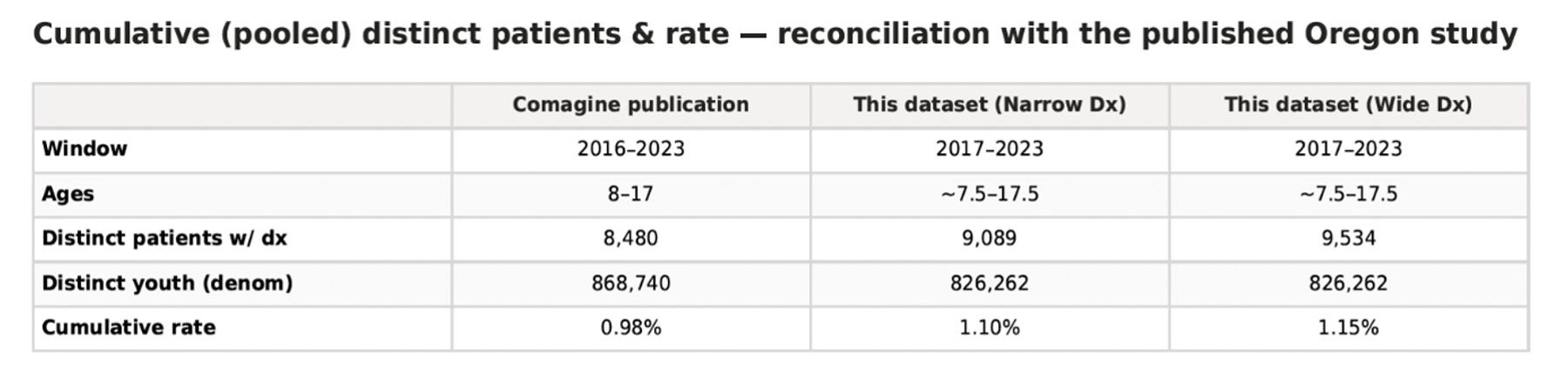
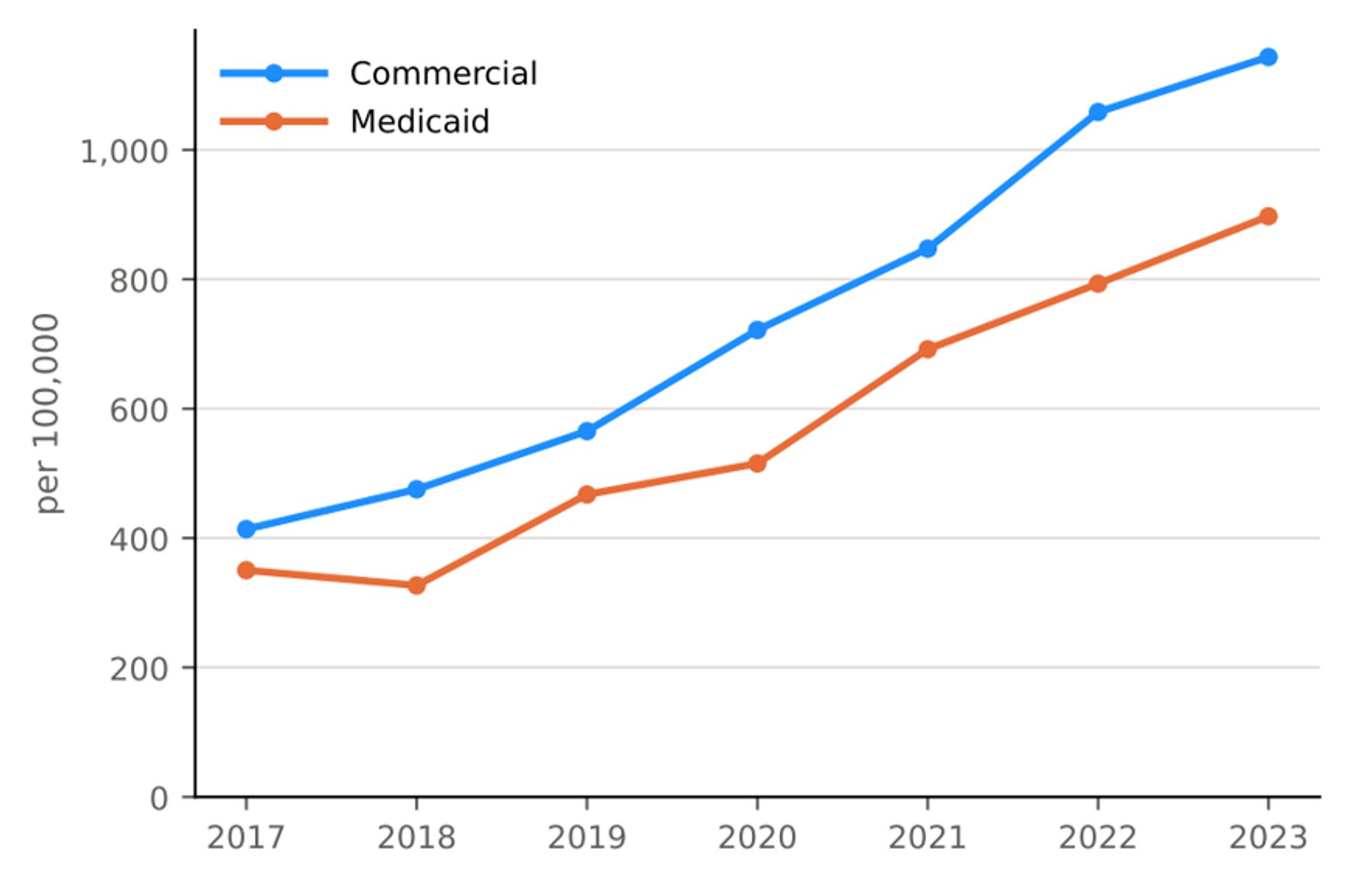
Table 1 summarizes how our data compare to those in the Research Connections study (the “Comagine publication” column). “Wide” represents all transgender-related diagnosis: F64 codes (“gender identity disorder”) as well as E34.9 codes (“endocrine disorder, unspecified”), which are also used in this context. “Narrow” represents F64 codes only. As the table shows, our data had a slightly higher percentage of diagnoses. One possible explanation for the difference is that our database has a more comprehensive set of commercial insurance data (around 90 percent vs. around 80 percent), and as Graph 1 shows, privately insured teens are diagnosed at higher rates than publicly insured teens. (The Research Connections study has a similar finding.) Further, since the Comagine data go back a year further than our data, and since the diagnostic prevalence rises over time (see below), it makes sense that a slightly shorter time frame would yield a slightly higher prevalence.
Table 1: Comparison of Comagine and MI data
Graph 1: Diagnostic trends, commercial versus public insurance
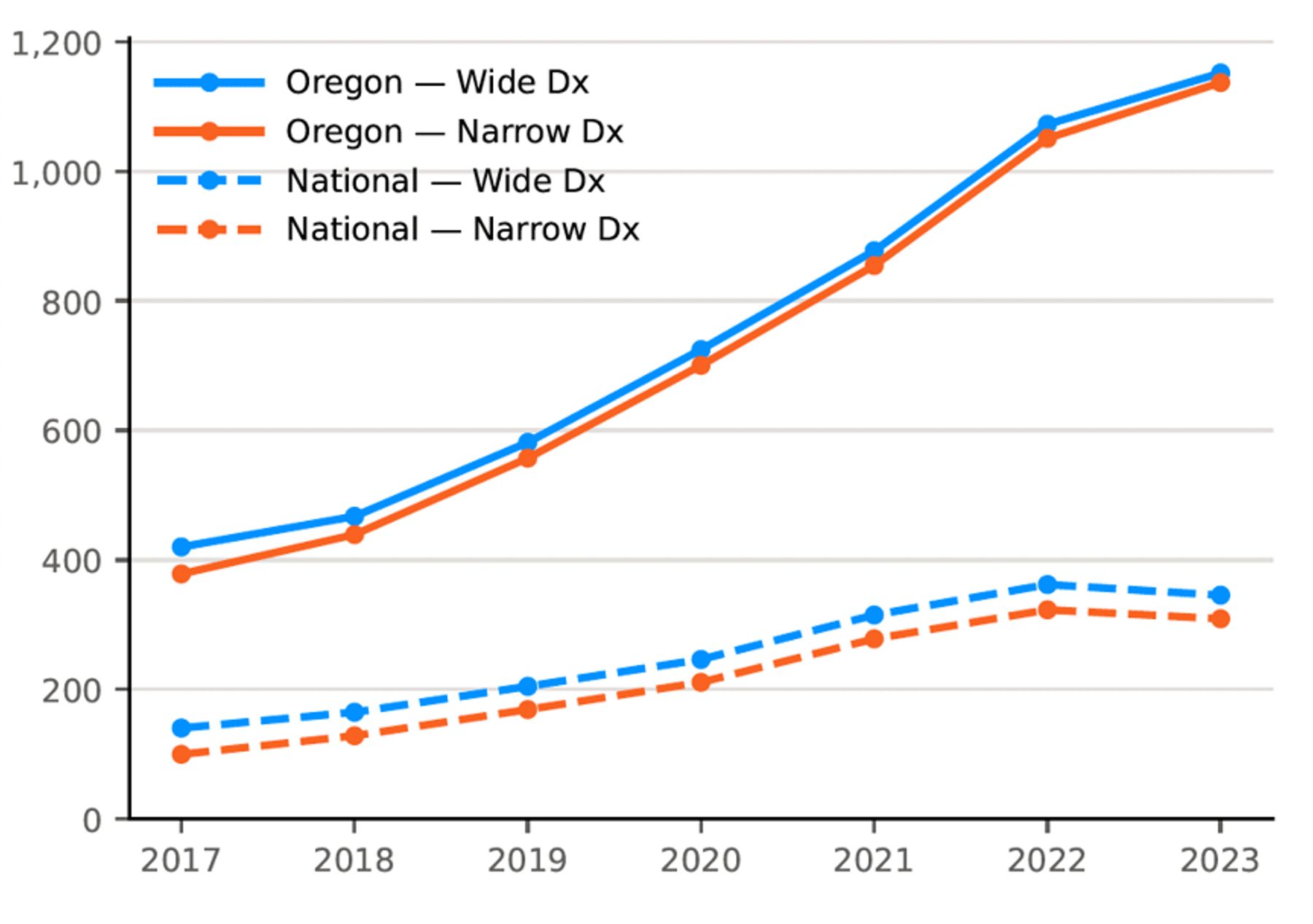
Graph 2 represents transgender-related diagnoses for minors (under 18) in Oregon compared to the national average over time, while Graph 3 represents transgender-related diagnoses among minors and young adults in Oregon broken down by age group. As the data show, diagnoses in adolescents were higher and rose faster in Oregon relative to the national average, and diagnoses in young adults were even higher than diagnoses in adolescents.
Graph 2: Diagnostic trends, Oregon versus national
Graph 3: Diagnostic trends in Oregon, by age group
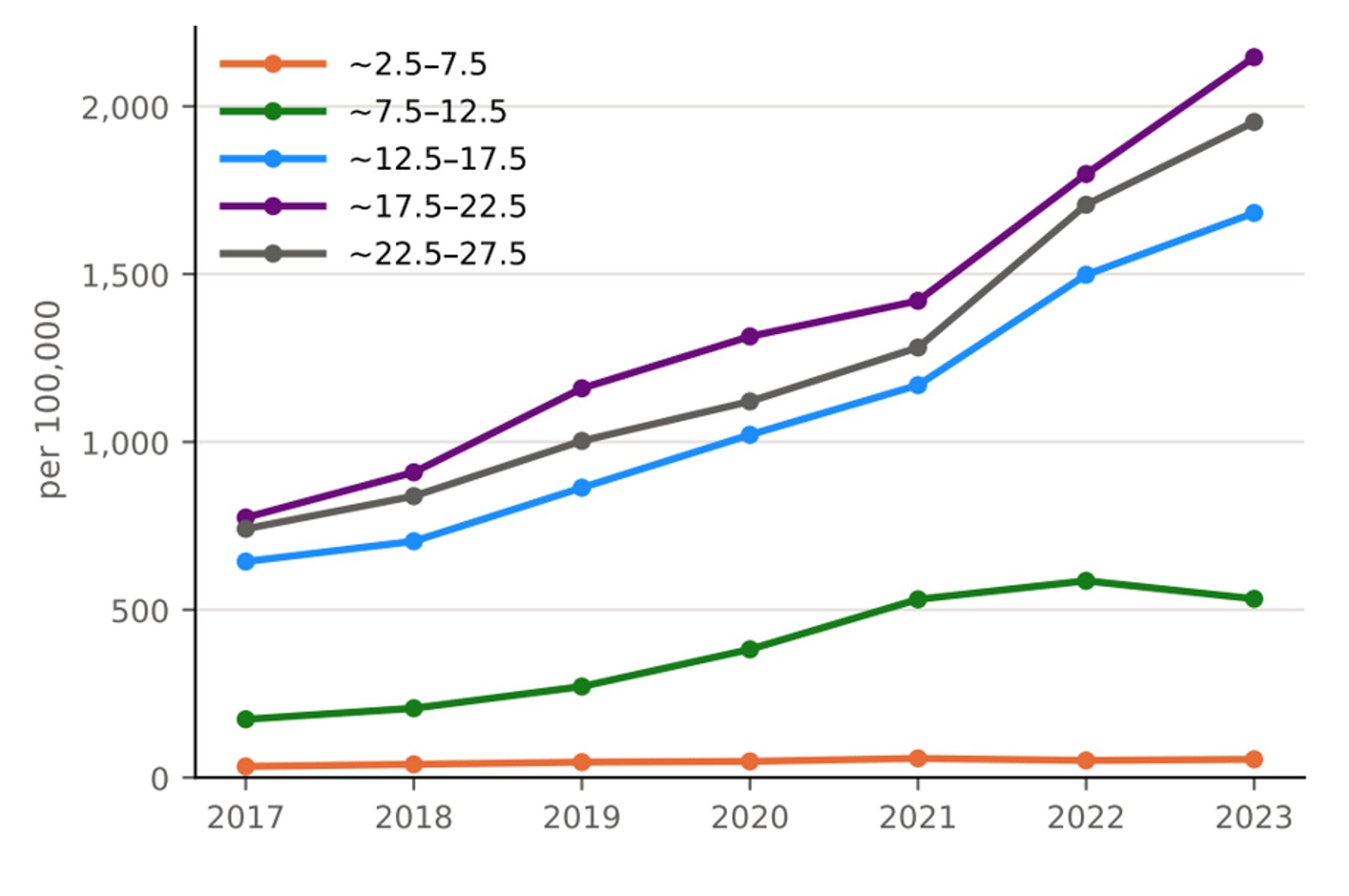
Chart 1 shows how Oregon (highlighted) compares with other states in terms of diagnostic prevalence in minors. Vermont tops the chart, with Oregon coming second. Along with Maine, these states had significantly higher diagnostic rates than other states. With a few notable exceptions, a state’s partisan leaning is a reasonable proxy for its diagnostic prevalence, with liberal states showing higher percentages than conservative states.
Chart 1: Diagnostic prevalence by state, 2023
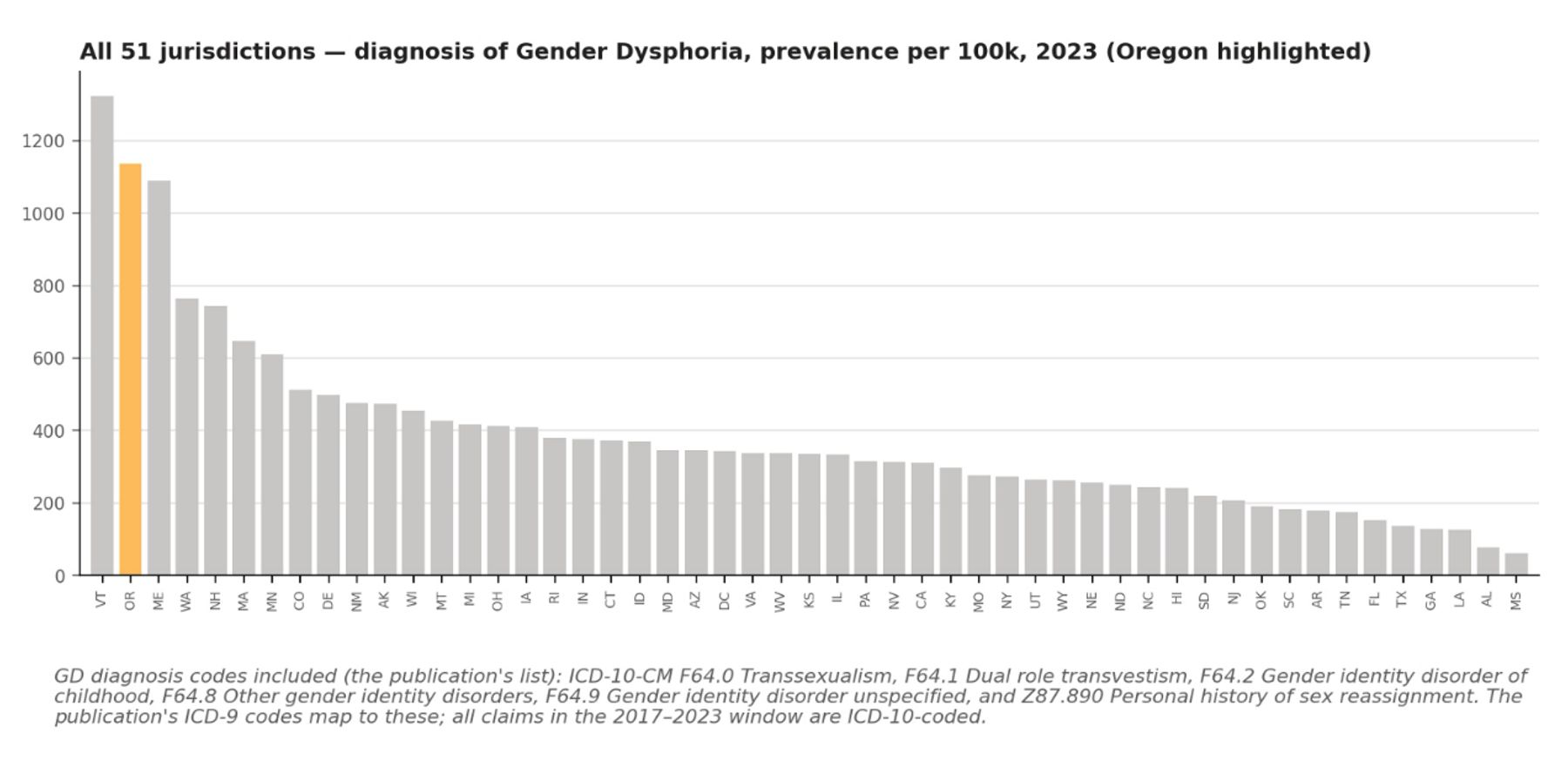
These findings weaken the claim long made by advocates of the “gender-affirming” model that cross-sex identity has a strong biological component. If it did, we would expect to see a more even distribution of diagnostic prevalence. Instead, minors in Vermont and Oregon were, respectively, 18 times and 16 times more likely than minors in Mississippi to have gender-related diagnosis, to give one example.
Our data support the alternative, sociogenic explanation for rising transgender identification in youth. That explanation would make sense especially in a state known for its very liberal culture. Another likely explanation for Oregon’s very high rates of diagnosis and medicalization is its embrace of the World Professional Association for Transgender Health’s “standards of care.” As Do No Harm’s Paul Terdal and I note in our Wall Street Journal piece, Oregon is the only state in the country to have formally adopted WPATH’s standards as the basis for its Medicaid coverage benefits.
The authors of the Research Connections study undoubtedly support the “gender-affirming” approach. For instance, they call hormonal interventions for minors “reversible” and “medically necessary,” and claim that they are “associated with better mental health and well-being.” Such statements defy all systematic reviews of the evidence to date; asserting them in this way betrays clear evidence of bias.
The authors also confidently assert that medical intervention “is individualized and provided within structured, multidisciplinary standards of care that recommend initiation of treatment only after appropriate diagnostic assessment, informed consent, and mental health considerations are addressed, with additional considerations for pubertal stage and fertility counseling.”
There are reasons to doubt the Research Connections authors’ confidence that medical intervention is given only after careful assessment. For one, their only citation for their claim is WPATH Standards of Care 8 (SOC-8). Even setting aside the scandals that erupted around the guideline’s creation, SOC-8 calls its assessment requirements “flexible,” and there is evidence, including from Oregon, that gender clinicians often disregard even its minimal criteria. For another, prominent advocates of the “gender-affirming” model have cited much lower diagnosis-to-medicalization ratios when reassuring the public that hormonal interventions follow rigorous assessment. For example, in a 2024 op-ed in the Boston Globe, Meredithe McNamara of the Yale School of Medicine cited figures in the 3 to 13 percent range to support her claim that medical intervention was “careful” and “slow-paced.” Compare this to Oregon, where, the new study finds, 22 percent of diagnosed girls and 28 percent of diagnosed boys were put on a medical pathway.
I asked Laura Edwards-Leeper, a child psychologist who co-founded the nation’s first pediatric gender clinic in Boston and who practiced in Oregon for over a decade, whether the Research Connections authors’ statement about careful assessment jibes with her experience. Edwards-Leeper said that it was “extremely troubling that the authors describe the medical care,” noting their failure to cite any evidence. Edwards-Leeper described a “cultural shift” during her time in Oregon, where “thorough assessment” that considered a “multitude of complex factors” related to patient history and mental health gave way to “treatment that prioritized young people’s autonomy and self-proclaimed identity.” (I previously interviewed Edwards-Leeper about her own assessment-based approach, which also has problems.)
Indeed, the authors’ own data on the social identification-to-diagnosis ratio should have been a red flag. As they note in the discussion section, “The proportion of adolescents receiving a [transgender]-related diagnosis in our sample was slightly lower than identity-based estimates for adolescents in Oregon (1.2 percent–3.2 percent).” They provide two citations, one showing 1.2 percent and the other showing 3.2 percent. The range is misleading, however: the 3.2 percent figure comes from a survey from 2024, whereas the data on which the authors rely was from 2016 to 2023. The 1.2 percent comes from the Williams Institute, a widely recognized authority in LGBT research, and draws from surveys conducted between 2017 and 2020, which coincides with the Comagine data.
To be sure, 1.2 percent seems like a low estimate for transgender identification among teens in a deep blue state like Oregon, and as the Research Connections authors go on to observe, national estimates are higher. But the authors seem to find the Williams Institute report credible. They presumably know that the 3.2 percent figure was outside their data range, and they write that the diagnosis rate “was slightly lower” than transgender identification in the state. Yet none of this triggers curiosity about the identification-to-diagnosis pathway.
The trends described above did not emerge organically. A series of steps, first taken by Oregon health authorities away from the public eye, and then continued by state Democrats, paved the way for Oregon to become a haven for transgender diagnoses and interventions.
Since 1994, Oregon has benefitted from a Section 1115 Medicaid waiver, a federal program administered by the Centers for Medicare and Medicaid (CMS) that exempts states from complying with key provisions of the Social Security Act if they can show they are implementing innovative health measures that lower costs and improve outcomes. To comply with Section 1115, the Oregon Health Plan (OHP), the state’s Medicaid system, draws up a “Prioritized List” of services, ranking them from most to least critical. Decisions about ranking are made by the state’s Health Evidence Review Commission (HERC), an interdisciplinary panel of experts, and must be based on “the clinical and cost effectiveness of services.”
In effect, Oregon’s waiver program makes it resemble European-style welfare states like Finland and Sweden, where a fiduciary duty to taxpayers, who fund health-care services, creates obligations on government to impartially evaluate the effectiveness of services. And just as would later happen in Finland and Sweden, in 2012 Oregon’s HERC evaluated the evidence for pediatric gender transition and found “very poor-quality evidence.” Unlike Finland and Sweden, however, HERC decided in 2014 to provide coverage for all transgender interventions for all patients—including top and bottom surgeries, even for children with no lower age limit—after listening to gender clinicians who testified that their practice was sound.
In 2023, Oregon Democrats passed HB 2002, which made Medicaid coverage of gender transition services for minors and adults mandatory, i.e., no longer dependent on HERC assessment. HERC was advised to endorse WPATH’s recommendations (SOC-8) as the minimal coverage standard. HERC assessed the evidence again, and again found it wanting. But intervention by gender clinicians at the Oregon Health and Science University ensured that HERC’s reluctance would not be a barrier. OHSU has been at the forefront of eliminating barriers to gender interventions and pioneering novel techniques designed to help young patients achieve body configurations “beyond the binary.”
In short, by any reasonable reading, Oregon, which received billions of dollars annually in Medicaid funding, is in violation of its Section 1115 Medicaid waiver, leaving it vulnerable to termination by CMS. HERC’s acknowledgment of the poor quality of evidence is not a matter of opinion. There is documented evidence for it, obtained through freedom of information requests.
There is a lot we still don’t know about Oregon. For example, of those who were diagnosed but did not receive hormonal interventions, how many wanted these interventions but were refused? Why do the commercially insured (presumably representing a higher social-economic status) have higher rates of diagnosis and medical intervention than the publicly insured? How do diagnostic and prescription practices differ by clinic or by provider? What effect, if any, have age minimum laws in red states had on the practice of gender medicine in Oregon?
Even without answers to these questions, however, the available data suggest a troubling story.